Simply what they did was to take two types of prostate cells, the basal and the luminal, tag them with surface tags, inject them into a mouse, and saw that only the basal cells grew, then they added two genes encoding for putative cancer pathways, and they saw that the basal cells grew to basal and luminal, like PIN, and then finally they added an AR, androgen receptor gene, and voila, prostate cancer. Result, showing how a specific pathway can generate cancer.
Let us go back and look at this a bit more.
1. First the prostate has cell collections which act as glands with basal cells at the base and luminal cells on top. The luminal cells secret to the gland, the luminal space. This we show below.

2. The normal prostate looks like what we show below, about 35-50 of these glands, and then surrounding material of muscle, blood supply, nerves, and lymphatics.

3. Now sometimes we see something called PIN, prostatic intraepithelial neoplasia, which is a growth of normal cells but not where they are to be. We may see the basal cells growing outwards and even some more luminal cells as well. The sign may be an increase in PSA since we have more luminal cells but the percent free PSA may stay high since the luminal cells are health ones. We show this below:

4. Then we may get prostate cancer, PCa, where the luminal cells types start to appear and grow without bound. The question is, where did these cells come from, other luminal cells or basal cells, or what. This is the question that the authors addressed with this elegant experiment. There is also the key question of whether it is just one cell that starts it or if the changed basal cells grow and if the environment switches many on over time. The latter effect is similar to that which has been observed in melanoma. Below we show what happens next,

Looking at the prostate as a whole we then may see what appears below. Namely we may see low grade cancer cells and then clusters of high grade cancer cells, this leads to the Gleason grading system.

5. Thus the question posed by the authors was the one which asks from what cell does cancer begin? Their answer suggests the basal cell.

6. Pathways have been studied for PCa extensively and one of the recent examples was in a 2003 NEJM article and is shown below.

But the authors took a simple approach and looked at three genes in the putative pathway process. This is shown below:
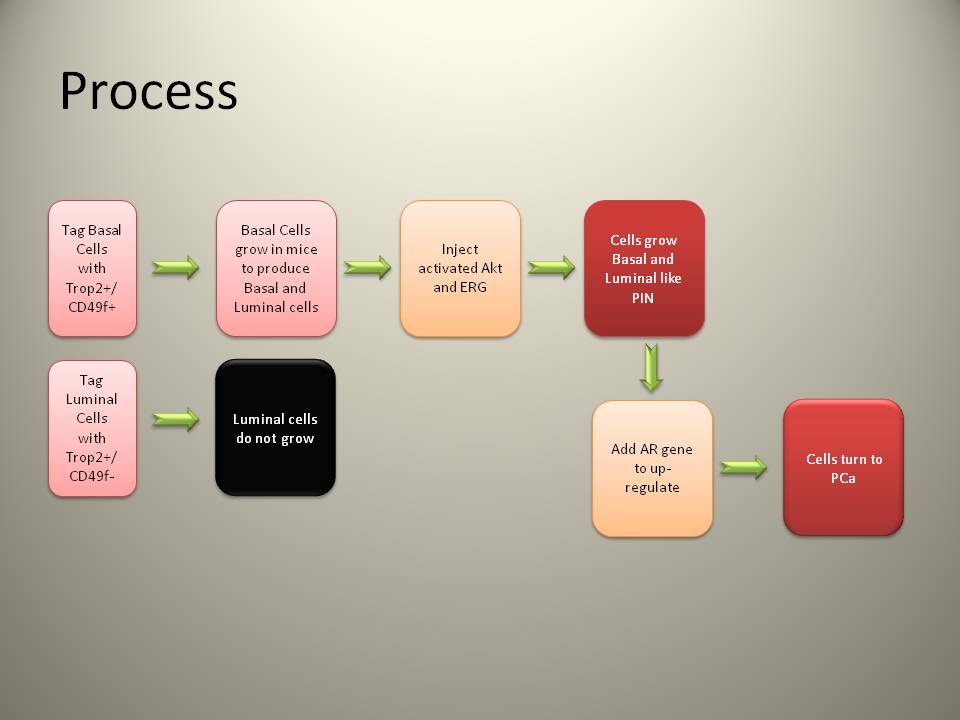
First they showed that only basal cell proliferate into both basal and luminal. Then they added ERG and Akt genes known as key in the pathways, and they obtained PIN, and then they added AR, the androgen receptor to drive the previous two genes and the result was PCa.
They were able to keep track of basal and luminal cells by tagging them with cell surface markers, as shown below. Basal was positive for both and luminal positive for one and negative for another, a good example of tracking the cells as the transform.

As to the two initial genes we have:
(i) Akt: There are in humans three genes in the "Akt family": Akt1, Akt2, and Akt3. These genes code for enzymes that are members of the serine/threonine-specific protein kinase family. Akt1 is involved in cellular survival pathways, by inhibiting apoptotic processes. Akt1 is also able to induce protein synthesis pathways, and is therefore a key signaling protein in the cellular pathways that lead to skeletal muscle hypertrophy, and general tissue growth. Since it can block apoptosis, and thereby promote cell survival, Akt1 has been implicated as a major factor in many types of cancer.
(ii) ERK: Extracellular signal regulated kinases, ERK, are protein kinase signalling molecules involved in the regulation of meiosis, mitosis, and postmitotic functions in cells.
This study still leaves several open questions:
1. Is the clonal theory of cancer still standing or can a single cell transform and then induce other cells via chemical signaling.
2. Is the basal cell the only one. There appears to be some issues here and the review article looks at these.
3. Is PIN an artifact or a precursor. Clinically men with PIN have a slightly higher risk of PCa but not a substantially higher as would be argued in this model. In fact men with PCa do not always have PIN and men with PIN do not always get PCa.
4. Is this just an artifact pathway, the true pathway, one of many pathways.
5. If we can duplicate pathways can we than better control the disease.
6. What does this tell us about detection and staging.
All in all this is just another step in telling us that we are still learning. And as to my favorite topic, Comparative Effective Clinical Research and the new Health Care Bill, well, it will never work!


